 Dear Colleague,
Dear Colleague,
"You can't connect the dots looking forward; you can only connect them looking backwards. You have to trust that the dots will somehow connect in the future."
This insight from IT visionary Steve Jobs has parallel in orthodontics. Orthodontics tends to focus on just the months during which treatment is given, but to truly connect the dots one may need to look back...way back.
Early Head and Face Deformation
Which is better, to treat a symptom or understand the root cause of the problem?
Of course, the answer is that by understanding the causes of a problem, one can design a more effective treatment rather than blindly addressing symptoms. In my journey toward better patient care I made the decision to focus on the causes of malocclusion before investing in yet another appliance system.
Hereditary factors are important in malocclusion, but one obvious cause is distortion of the head and face before, during, and after birth. Osteopaths claim that nearly 90% of births show some form of cranial distortion. Allopathic pediatricians do not put the percentage as high but do agree that distortion of the cranium in newborns is common. For a good primer on how pediatricians think about head deformation I recommend the following link to the Craniofacial Program at the world-renowned Hospital for Sick Children in Toronto (click here).
To gain some idea of cranial distortions that can occur even in a normal birth I recommend browsing through Google Images which you can access here (click here). Facial distortion resulting from the cranial deformations is conspicuous in a number of the online examples.
For many years I did not make the connection between cranial and facial deformations in new born infants and their persistence into adulthood. I assumed distortions were temporary and would disappear with growth. This assumption was incorrect; some of these early distortions continue into adulthood. An orthodontic diagnosis should include identifying these distortions and the effects they may have had on the face and dentition.
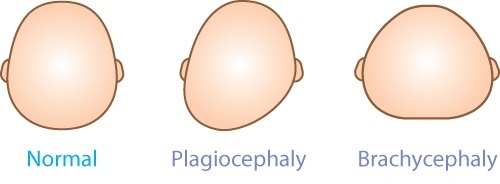
Where it is conspicuous in an infant, pediatricians describe it as plagiocephaly or brachycephaly, depending on the nature of the deformation. They may recommend that parents condition the infant through specific physical exercises or use specialized bedding to help mould the infant head. In more severe cases, a specially designed helmet may be prescribed for three to six months to reshape the cranium.
The Angle classification of malocclusion is still the predominant system used in orthodontics. The cranial base is viewed as a relatively stable structure from which various facial and dental features can be analyzed through a lateral head radiograph. The emphasis has been on a two-dimensional approach. The significance of facial asymmetry is often missed resulting in treatment creating an excellent dental result, but in a face that is far from balanced.
In contrast, the osteopathic classification is a sophisticated, three-dimensional approach which sees cranial and facial features as integral components of the whole body. The identification of a particular cranial strain or combination of strains is invaluable in reaching a diagnosis and in orthodontic treatment planning, since these forces—if not addressed—may continue to undermine treatment results long after treatment is complete.
I believe it is inevitable the usefulness and logic of the osteopathic approach will eventually supersede the traditional Angle system. It is my intention to provide evidence of its theoretical and clinical superiority in future communications.
Gavin

Leave a Reply
You must be logged in to post a comment.