
For over a century the classification system pioneered by Edward Angle has been central to the way dentists and orthodontists visualize patients and treatment planning. Orthodontists are well aware of the shortcomings of the Angle classification system for teeth but have lacked a better alternative.
My passion has been to develop a clinical orthodontic approach that takes advantage of the body’s innate ability to heal, whatever the patient’s age. On my journey, I have been compelled to find ways to integrate new developments in biology. The challenge has been to best fit these advances into a workable clinical protocol. My experiences with TMJ diagnosis and treatment offered me tantalizing clues that a better classification model might be possible.
TM joint dysfunction, was once an avant-garde, esoteric area of specialization before it entered the mainstream of dental and orthodontic practice. Thirty years ago I attended seminars by leaders in the TMJ field and reflected on my own work with my patients. I realized the assessment and management of orthodontic patients and TMJ patients have much in common. Whether the patient is a young child, an adolescent, or an adult—either with or without TMJ symptoms—the same basic diagnostic principles apply.
In the 1980s I developed a clinic dealing primarily with TMJ problems. This included physical therapists, several of whom had cranial osteopathy. I was intrigued by what they were doing—their approach was simultaneously foreign but oddly familiar. One osteopathic best practice made perfect sense to me—the osteopathic classification of cranial shapes. This system can easily be extended to include the face and the teeth. Each cranial variation, or strain to use the osteopathic term, tends to have certain facial and dental characteristics.
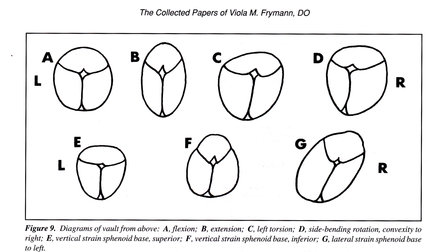
As I became more familiar with this cranial classification system, it has become an essential and practical addition to my diagnostic toolkit. Figure 1 is taken from a landmark osteopathic article on strains found in 1,250 newborn infants. Almost 90% of the infants had cranial distortions of some kind when seen in the days immediately following their birth. Given the trauma of birth this is not surprising. Follow-up studies show these strains tend to resolve spontaneously as the infant begins to suckle but in many cases some degree of distortion may persist. These distortions are a major source of malocclusion.
In my opinion, the osteopathic classification of cranial strains is a radical improvement over the Angle classification. It makes sense of the facial and dental variations by connecting the cranial, facial and dental features in a logical way. I will show examples of this in future cases reports.
In the meantime, I am happy to share a series of articles on how cranial strains affect the face, mouth and teeth. I co-authored these articles with my friend and colleague Dr. Dennis Strokon. These articles are freely available from my website for registered readers. As far as I know, they are the only existing source of information that deals with this subject in a systematic way.
I welcome you to join me as I continue to explore how a more integrative approach to dental and orthodontic practice can yield better, more lasting results and contribute to our patients’ overall well-being.
Gavin

Leave a Reply
You must be logged in to post a comment.